Real-Time Haemodynamic Responses to Yoga Asanas and Pranayama: A Cardiac Imaging Study
By Observed and Reported by: Dr. S. Thanikachalam, MD, DM (Cardiology), DSc (Honoris Causa), Padma Shri Awardee
Date of Study: 21 December 2006
Real-Time Haemodynamic Responses to Yoga Asanas and Pranayama: A Cardiac Imaging Study
Observed and Reported by: Dr. S. Thanikachalam, MD, DM (Cardiology), DSc (Honoris Causa), Padma Shri Awardee
Chairman & Director, Cardiac Care Centre, Sri Ramachandra Medical College & Research Institute (SRMC & RI), Chennai
In Collaboration with: Dr. Asana Andiappan and the Andiappan Yoga Research Team (Yogananth Andiappan, Lakshmi Andiappan, T A Krishnan.)
Foreword: Why This Collaboration Mattered
When Dr. Asana Andiappan and his yoga team approached our institution to conduct a structured yoga research study on various asanas and pranayamas, I received the proposal not as a novelty, but as a scientific homecoming.
In 1979, our own team at Madras Medical College published what may have been one of the earliest peer-reviewed studies documenting the long-term cardiovascular effects of yoga — specifically its benefits in patients with hypertension and coronary artery disease. That paper, published in the Journal of the Association of Physicians of India, was received with cautious interest at a time when the medical community remained largely sceptical of yoga's therapeutic potential. Nearly five decades later, the landscape has transformed dramatically. What our 1979 paper suggested — that yoga produces measurable, durable cardiovascular benefit — is now corroborated by hundreds of clinical trials, systematic reviews, and population-level studies.
What remained scarce, however, was real-time physiological imaging data captured during active yoga performance under medical supervision — the kind of moment-to-moment haemodynamic documentation that only modern echocardiography and Doppler technology can provide. This is what Dr. Andiappan's collaboration made possible at our centre. As someone trained at Tufts University, Boston in Doppler, Colour Doppler, and transesophageal echocardiography, and as Past President of the Indian Academy of Echocardiography, I was perhaps uniquely placed to bring this imaging capability to a yoga research setting.
The study presented here is, to our knowledge, among the few in Indian medical literature to document live echocardiographic and Doppler responses across a comprehensive range of yoga postures, breathing techniques, bandhas, and kriyas — captured before, during, and immediately after each practice under continuous clinical monitoring.
The Growing Medical Case for Yoga Therapy
The acceptance of Yoga Therapy within mainstream medical science has gained considerable momentum over the past two to three decades, and has notably accelerated in the past two to three years. What was once relegated to the fringes of complementary medicine now occupies a respected position within cardiology, neurology, endocrinology, and psychiatry research worldwide.
As a clinician who has spent over five decades managing cardiovascular disease — from acute myocardial infarction to chronic hypertension, from valvular heart disease to cardiac rehabilitation — I can say with confidence that this shift is not merely cultural. It is evidence-based. Each component of yoga — asana, pranayama, bandha, kriya, dhyana — has demonstrable physiological consequences, and the published scientific literature now firmly supports what traditional practitioners have understood intuitively for centuries.
The conditions for which yoga therapy has demonstrated benefit, supported by published scientific evidence, include:
- Systemic hypertension — through parasympathetic activation, reduction in sympathetic tone, and improved baroreceptor sensitivity
- Angina pectoris and coronary artery disease — via reduced myocardial oxygen demand and improved endothelial function
- Myocardial infarction — as an adjunct in cardiac rehabilitation, improving exercise tolerance and reducing recurrence risk
- Diabetes mellitus — through enhanced insulin sensitivity and improved glycaemic regulation
- Obesity — by improving metabolic rate and autonomic balance
- Headache and migraine — via modulation of the autonomic nervous system and reduction in cortisol levels
- Anxiety neurosis and stress-related conditions — consistently among the best-documented benefits of yoga, mediated through HPA axis regulation
- Drug addiction — as an adjunct to behavioural therapies
- Bronchial asthma — through pranayama-driven improvements in lung mechanics and respiratory muscle strength
- Premenstrual syndrome — via hormonal and autonomic modulation
- Hypercholesterolaemia — with documented reductions in LDL and total cholesterol with regular practice
- Pregnancy — through safe improvements in physical conditioning and stress reduction under guidance
- Acute and chronic stress — through parasympathetic dominance and cortisol reduction
- Arthritis — via isometric muscle toning without excessive joint loading
- Epilepsy — emerging evidence suggests autonomic modulation may reduce seizure frequency
Beyond disease management, a consistent yogic lifestyle confers an overall improvement in quality of life, physical fitness, work output, memory, and concentration — benefits that extend well beyond any single organ system.
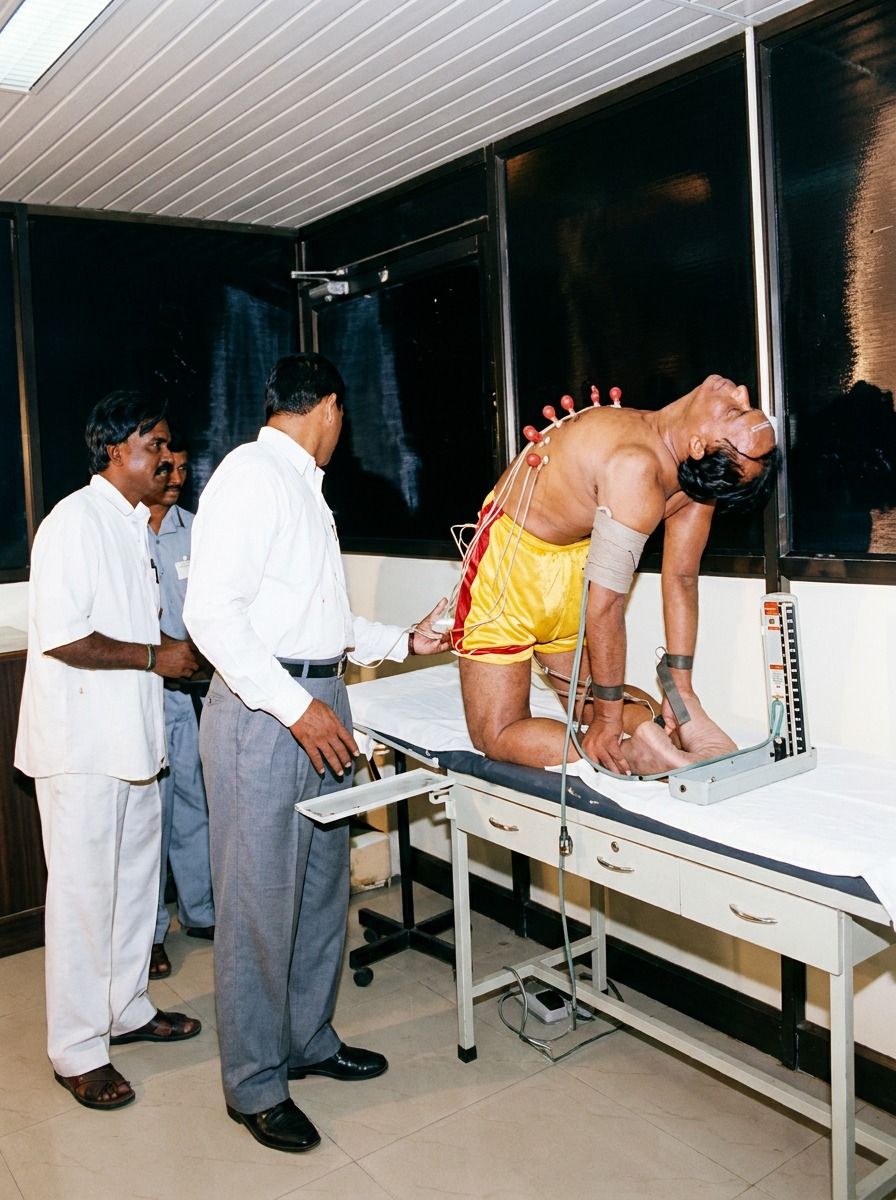
Study Design: What We Measured and How
Dr. Andiappan's team performed a series of yoga asanas, pranayamas, bandhas, and kriyas at our Cardiac Care Centre under direct medical supervision. For each practice, the following parameters were recorded systematically:
- Blood pressure (systolic and diastolic), pulse rate, and respiratory rate — measured before, during, and after each asana
- Echocardiographic imaging — including assessment of left ventricular (LV) and left atrial (LA) cavity dimensions in real time
- Doppler flow measurements — across the mitral, tricuspid, and aortic valves
- Carotid Doppler — to assess cerebral perfusion dynamics during inverted and semi-inverted postures
- Internal jugular vein Doppler — to document venous return dynamics in postural inversions
This multi-modal cardiac imaging approach — using both structural and flow-based assessment simultaneously — was central to extracting the haemodynamic meaning from each posture. The value of this methodology lies not in any single measurement, but in the integrated picture it provides of how the human body interacts with the cardiovascular system during active yoga practice.
Haemodynamic Findings: Asanas and the Cardiovascular Response
Cardiovascular Parameters During Standard Asanas
Across all asanas performed without deep breathing components, a consistent pattern emerged: a moderate, self-limiting increase in heart rate of approximately 10 beats per minute and in systolic blood pressure of approximately 10 mmHg. This is a physiologically meaningful but clinically benign response — far more modest than that observed during equivalent levels of dynamic exercise.
In asanas such as Halasana and Yoga Mudra, an additional rise in diastolic blood pressure of approximately 10 mmHg was observed. This diastolic response is characteristic of isometric-type loading, in which muscle contraction compresses peripheral vasculature and transiently increases systemic vascular resistance. Importantly, both systolic and diastolic pressures returned to baseline within one minute of cessation of the posture — a finding that reflects intact autonomic recovery and validates the safety of these postures in supervised settings.
Before and after all asanas, respiratory rate showed an average increase of approximately 4 breaths per minute — a modest but consistent rise consistent with the mild metabolic and ventilatory demands of postural performance.
Doppler Valve Flow in Resting and Gentle Postures
Following the haemodynamic recordings, cardiac imaging with Doppler flow assessment across the mitral, tricuspid, and aortic valves was performed where technically feasible. Asanas such as Savasana (corpse pose) and Padmasana (lotus pose) produced no appreciable alteration in Doppler flow measurements. This is consistent with their well-recognised roles as rest and meditative postures, placing minimal haemodynamic demand on the heart while facilitating parasympathetic dominance and sympathetic withdrawal.
The Bandhas and Kriyas: A Unique Cardiovascular Window
Among the most scientifically illuminating observations of this study were those made during the performance of bandhas (internal locks) and kriyas (cleansing techniques) — specifically Nauli (abdominal rolling), Uddiyana Bandha (upward abdominal lock), and Maha Bandha (the great lock).
The unconventional body positions and wide thoracic excursions involved in these practices made continuous Doppler valve imaging technically impossible during active performance. To circumvent this methodological challenge, we directed our imaging assessment to the LV and LA cavity dimensions — parameters that can be reliably obtained even under suboptimal acoustic windows.
The finding was unambiguous: all three of these practices produced an acute, uniform reduction in both LV and LA cavity size, accompanied by an increase in heart rate, with complete return to normal chamber dimensions upon cessation of the practice.
The physiological explanation is both straightforward and elegant. During these practices, two powerful mechanisms converge to temporarily reduce venous return to the heart:
- Rapid, forceful exhalation breathing — as seen in Nauli — creates marked fluctuations in intrathoracic pressure. The expiratory phase transiently increases intrathoracic pressure, impeding venous return through the inferior and superior vena cava.
- Forceful contraction of the abdominal wall toward the spine — the defining action of Uddiyana Bandha — effectively compresses the abdominal venous reservoir, reducing the volume of blood available for cardiac filling.
Together, these mechanisms produce the acute decrease in LV and LA size we observed — a direct imaging correlate of reduced cardiac preload. The immediate restoration of normal chamber size upon ending the practice confirms that this is a transient, reversible, and physiologically controlled phenomenon. These techniques act like a bellows that first compresses and then releases, ultimately creating a brisk restoration of venous return that enhances cardiac filling after the procedure.
Jugular Venous Dynamics in Inverted Postures
Among the most visually striking findings in this study was the behaviour of the internal jugular veins during Viparita Karani (legs-up- pose) and Halasana (plough pose).
During both postures, real-time imaging demonstrated an acute bilateral dilation of the internal jugular veins, accompanied by markedly reduced Doppler flow velocity within the veins. Upon return to the normal upright or supine position, the Doppler flow velocity in both jugular veins rose to levels notably exceeding their pre-posture baseline — a rebound that represents an accelerated restoration of venous drainage toward the heart.
The mechanism is mechanical in nature. In both postures, the cervical venous pathway is placed in a state of acute positional compression — a transient buckling of the internal jugular veins. Gravity, combined with the angular load imposed by the posture on the neck and thoracic inlet, impedes the normal drainage gradient from the head toward the superior vena cava. The vein distends proximally while flow velocity falls distal to the point of compression.
The supranormal rebound flow velocity upon posture cessation confirms this is a benign, self-resolving phenomenon in healthy practitioners. It is worth noting that during both these postures, carotid Doppler flow showed no appreciable change — an important finding that distinguishes jugular venous dynamics from arterial cerebral perfusion, and provides reassurance regarding the maintenance of cerebral blood delivery throughout these postures.
Sirsasana: Cerebrovascular Autoregulation in Action
The haemodynamic profile of Sirsasana (headstand) deserves particular attention, as it represents the most physiologically complex of the postures studied.
Unlike the jugular veins — which showed marked postural changes — carotid Doppler flow during Sirsasana did not show an immediate or proportional change. Instead, after a lag period of approximately 30 seconds, the diastolic flow velocity in both carotid arteries increased appreciably compared to the pre-posture resting baseline. Following cessation of the posture, a recovery period of at least 30 seconds was required before carotid diastolic flow returned to its normal level.
This finding is a direct clinical demonstration of cerebrovascular autoregulation — the brain's intrinsic capacity to maintain adequate perfusion despite changes in posture, blood pressure, and gravitational orientation. The 30-second lag represents the time required for the cerebral vasculature to sense the altered perfusion pressure induced by inversion and respond by reducing cerebrovascular resistance, resulting in a maintained and modestly enhanced cerebral diastolic perfusion during sustained Sirsasana.
The 30-second recovery time after cessation of the posture suggests that the cerebrovascular system, while adaptive, requires a brief period of reorientation after returning from full inversion. From a practical standpoint, this argues against performing Sirsasana in rapid or repeated succession without adequate intervening rest — a consideration that teachers and practitioners should incorporate into safe sequencing.
Notably, Sirsasana produced no appreciable change in systolic blood pressure. The increase in diastolic carotid flow velocity is therefore most plausibly attributed to a fall in cerebrovascular resistance in response to the inverted posture — a passive, autoregulatory response rather than a pressure-driven phenomenon.
Yoga Versus Dynamic Exercise: A Cardiologist's Perspective
One of the most practically valuable insights from this study is what it reveals about how yoga differs from conventional dynamic exercise as a cardiovascular stimulus. This distinction is clinically important because it determines where yoga fits within the broader landscape of cardiac rehabilitation and preventive cardiology.
In dynamic exercise — walking, cycling, swimming — the cardiovascular response is characterised by a linear, progressive rise in heart rate and systolic blood pressure proportional to exercise intensity and duration. The predominant driver of increased cardiac output in dynamic exercise is vasodilation in the working muscles, which dramatically reduces peripheral resistance and, in combination with vigorous respiratory activity, markedly increases venous return to the heart.
Yoga asanas operate by fundamentally different mechanisms:
- Most asanas are isometric or quasi-isometric in nature — they tone and compress muscle groups rather than rhythmically shortening and lengthening them. Isometric contraction squeezes muscle fibres and the venules running through them, facilitating local venous emptying without the peripheral vasodilation characteristic of dynamic exercise.
- The heart rate and blood pressure response to asanas is modest and non-progressive — it does not escalate with the duration of posture holding the way that dynamic exercise drives a linear cardiovascular response.
- Asanas involving deep breathing act as bellows — generating cycles of negative and positive intrathoracic pressure that first transiently reduce venous return and then, at the conclusion of the practice, create a brisk and augmented restoration of venous return to the heart.
The net effect across most asanas is this: yoga tones the segmental muscles that serve as peripheral venous pumps, optimises local venous drainage, and then — at the moment of posture release — facilitates a gushing restitution of arterial blood flow into the limb vasculature and venous return into the cardiac chambers.
This mechanism has a direct clinical implication. For individuals who cannot safely undertake aerobic exercise — those in the early post-myocardial infarction period, older patients with joint limitations, or those with exercise-limiting angina — yoga's isometric toning mechanism offers a medically viable pathway to maintain peripheral vascular tone, support venous return, and preserve cardiovascular conditioning. Yoga does not replace aerobic exercise; rather, it complements it by engaging vascular and autonomic pathways that conventional exercise does not reach in the same way.
Meditation, the Neuroendocrine System, and the Heart
In the past three decades, a considerable body of medical research has been dedicated to understanding the physiological mechanisms by which meditation exerts its well-documented clinical benefits. The cardiovascular system, in particular, has been studied in depth — with investigators examining the effects of sustained meditative practice on heart rate variability, baroreflex sensitivity, autonomic tone, and endothelial function.
What is now well-established is that stress-related cardiovascular conditions are among those most consistently and significantly benefited by meditation. The mechanisms are multiple:
- Sustained meditation reduces cortisol and other stress hormones secreted by the HPA axis, directly lowering the adrenergic drive that elevates heart rate and blood pressure in response to psychological stress.
- Regular meditative practice increases parasympathetic tone and reduces sympathetic dominance, shifting the autonomic balance in a cardioprotective direction.
- These neuroendocrine changes translate into measurable clinical outcomes: lower resting blood pressure, reduced heart rate, improved heart rate variability, and a blunted cardiovascular response to acute stressors.
The cardiovascular adaptations we documented during the asana and pranayama components of this study can be understood as the acute, session-level expressions of the same physiological remodelling that meditation produces over months and years of sustained practice. Asanas and pranayamas prepare the body; meditation consolidates the benefit at the level of the autonomic nervous system and the neuroendocrine axis.
Closing Observations
What Dr. Andiappan and his team demonstrated in our cardiac imaging laboratory was not mysticism. It was measurable physiology — visible in real time on the echocardiography and Doppler screen, reproducible across multiple postures, and consistent with well-established cardiovascular science.
The haemodynamic changes we documented — the transient reduction in LV and LA cavity size during bandhas, the jugular venous distension and rebound in inversions, the autoregulatory carotid diastolic response during Sirsasana, the modest and self-limiting blood pressure responses across asanas — all speak to a system of practices that engages the cardiovascular apparatus in a sophisticated, controlled, and ultimately beneficial manner.
For the generation of cardiologists that follows, I offer this observation: the data needed to integrate yoga into evidence-based cardiovascular medicine is no longer absent. It is accumulating rapidly. What is now required is the institutional willingness to bring yoga into the cardiology ward — not as an alternative to conventional therapy, but as an adjunct with documented, imaging-confirmed physiological mechanisms.
The present collaboration between Dr. Andiappan's yoga research team and our cardiac centre represents precisely the kind of interdisciplinary work that will build that evidence base and, ultimately, benefit the patients we serve. As a cardiologist who first studied yoga's effects on the heart in 1979, and who has now had the privilege of watching those effects unfold in real time under Doppler imaging, I can say with conviction: the science has caught up with the practice. It is time for clinical medicine to follow.
Dr. S. Thanikachalam, MD, DM (Cardiology), DSc (Honoris Causa), Padma Shri Awardee
Chairman & Director, Cardiac Care Centre, SRMC & RI, Chennai
In collaboration with Dr. Asana Andiappan and the Andiappan Yoga Research Team